Overview
Plantar fasciitis accounts for nearly 15% of foot-related complaints in general practice (Riddle & Schappert, 2004). As a leading cause of heel pain, it frequently affects adults aged 40–60 and is often managed conservatively. Physiotherapy plays a central role in achieving symptom resolution and preventing recurrence.
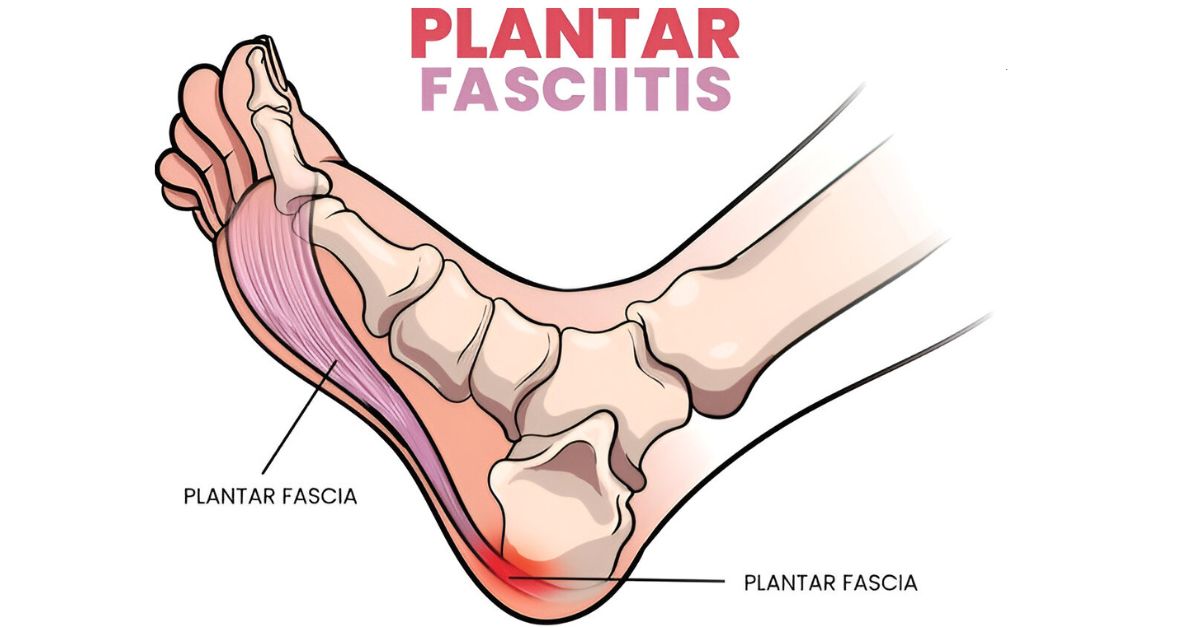
Pathophysiology
Histological studies reveal a degenerative rather than inflammatory process in most chronic cases, with collagen disorganization and microtears in the fascia. Contributing factors include:
- Excessive foot pronation or supination
- Gastrocnemius-soleus tightness
- Altered gait biomechanics
- Poor load distribution due to weak intrinsic foot musculature
Evidence-Based Physiotherapy Interventions
A multi-modal approach targeting flexibility, load management, and strength is supported by several high-quality RCTs:
- DiGiovanni et al. (2003) conducted a prospective RCT showing that tissue-specific plantar fascia stretching was significantly more effective than standard Achilles stretching in reducing heel pain and improving function.
- Rathleff et al. (2014) demonstrated that patients who followed a high-load strength training protocol (progressive calf raises with forefoot elevation) experienced superior long-term outcomes compared to those performing stretching alone. At 3 months, the strength group showed significantly greater improvements in pain and foot function indices.
- Huffer et al. (2017) found that manual therapy combined with exercise led to superior outcomes in both pain reduction and disability compared to exercise alone in a randomized trial.
Our Physiotherapy Protocol Includes:
- Plantar fascia-specific stretching (diGiovanni method)
- Progressive loading exercises, including eccentric heel raises
- Manual therapy for ankle dorsiflexion restriction
- Soft tissue mobilization of the calf and plantar fascia
- Footwear modification and custom taping or orthotics
- Education on load management and return-to-activity strategies
When to Refer
- Physiotherapy is appropriate at any stage but particularly indicated when:
- Symptoms persist beyond 2–4 weeks of self-care
- There is recurrent or chronic pain (>3 months)
- Foot biomechanics suggest need for movement re-education
- The patient is not responding to NSAIDs or corticosteroid injections
Conclusion
Plantar fasciitis responds exceptionally well to conservative physiotherapy when treatment is based on current evidence. Our goal is to work collaboratively with physicians to reduce pain, improve function, and prevent recurrence through a tailored, patient-centered approach.
References:
DiGiovanni, B. F., Nawoczenski, D. A., Lintal, M. E., Moore, E. A., Murray, J. C., Wilding, G. E., & Baumhauer, J. F. (2003). Tissue-specific plantar fascia-stretching exercise enhances outcomes in patients with chronic heel pain: A prospective, randomized study. Journal of Bone and Joint Surgery, 85(7), 1270–1277. https://doi.org/10.2106/00004623-200307000-00003
Rathleff, M. S., Molgaard, C. M., Fredberg, U., Hansen, K. M., & Ahrendt, P. (2014). High-load strength training improves outcome in patients with plantar fasciitis: A randomized controlled trial with 12-month follow-up. Scandinavian Journal of Medicine & Science in Sports, 25(3), e292–e300. https://doi.org/10.1111/sms.12313
Huffer, D., Hing, W., Newton, R., & Clair, M. (2017). Strength training alone versus combined strength and manual therapy in the treatment of plantar fasciitis: A randomized controlled trial. Journal of Science and Medicine in Sport, 20(10), 962–968. https://doi.org/10.1016/j.jsams.2017.03.011
Riddle, D. L., & Schappert, S. M. (2004). Volume of ambulatory care visits and patterns of care for patients diagnosed with plantar fasciitis: A national study of medical doctors. Foot & Ankle International, 25(5), 303–310. https://doi.org/10.1177/107110070402500505