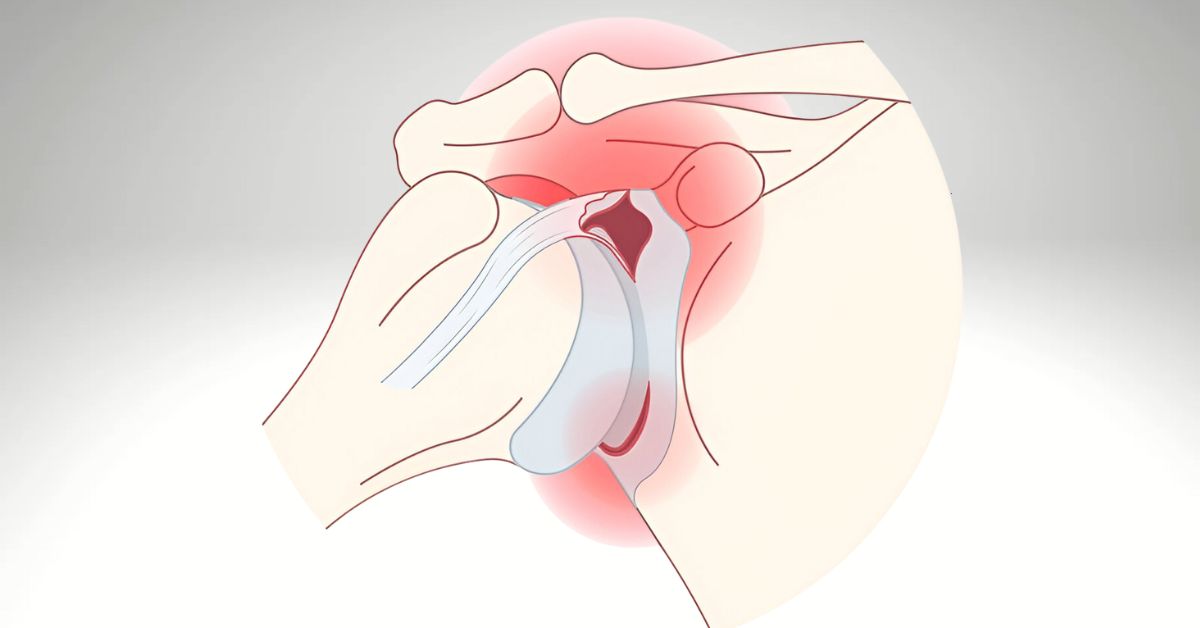
Types of shoulder labral tears (SLAP, Bankart) and indications for physiotherapy.
Shoulder Labral Tears: Evidence-Based Conservative Management through Physiotherapy
Introduction Shoulder labral tears, including SLAP (superior labrum anterior-posterior) lesions and Bankart lesions, are commonly encountered in athletes and active adults. These injuries, often resulting from trauma or repetitive overhead…