Introduction
Shoulder labral tears, including SLAP (superior labrum anterior-posterior) lesions and Bankart lesions, are commonly encountered in athletes and active adults. These injuries, often resulting from trauma or repetitive overhead motion, contribute to shoulder instability, dysfunction, and pain.
While arthroscopy remains a treatment option for complex tears, high-quality RCTs support conservative management through physiotherapy for selected patients—often resulting in comparable or superior long-term outcomes.
Pathophysiology and Classification
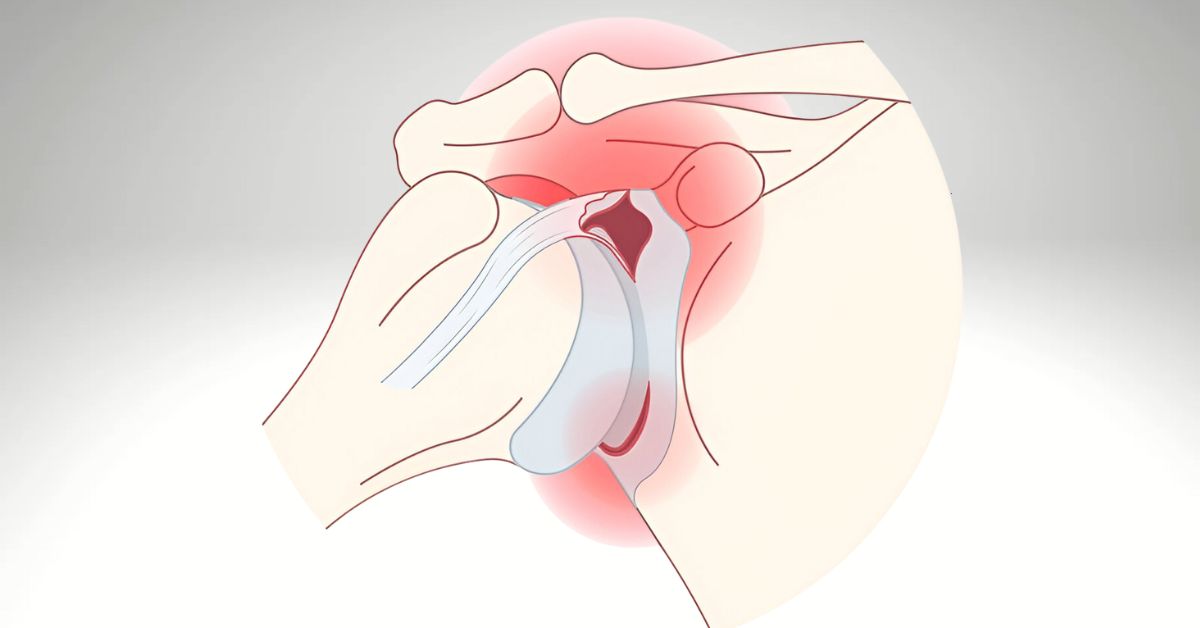
- The labrum deepens the glenoid cavity and provides a suction seal for joint stability. Tears may be classified as:
- SLAP lesions (often from overhead activities or traction injuries)
- Bankart lesions (associated with anterior dislocations)
- Degenerative labral fraying in older populations
RCT-Supported Physiotherapy Interventions
1. Structured Rehabilitation vs. Surgery
- Kim et al. (2018) compared non-operative physiotherapy to surgical intervention in patients with SLAP tears. The non-surgical group, which followed a 12-week progressive physiotherapy plan, demonstrated equivalent improvements in pain and function at 6 months without surgical risks.
- Key rehab components: rotator cuff strengthening, scapular stabilization, neuromuscular control, and proprioceptive retraining.
2. Joint Hypermobility and Labral Integrity
- Falla et al. (2014) found that even patients with joint laxity and confirmed labral lesions experienced improved joint control, reduced subluxation, and better pain management through targeted physiotherapy—suggesting structural lesions are not always primary drivers of dysfunction.
3. Prevention of Surgery and Delayed Recovery
- Schroeder et al. (2016) demonstrated that early physiotherapy following a labral injury reduced time lost from work and improved early return to sport compared to delayed intervention.
Clinical Implementation: Our Physiotherapy Approach
- Phase I: Reduce inflammation, normalize scapular positioning, limit aggravating activities
- Phase II: Restore ROM, begin dynamic stability, address kinetic chain deficits
- Phase III: Rotator cuff and scapular strengthening, proprioceptive retraining
- Phase IV: Gradual return-to-sport-specific drills or job-specific loading
We utilize tools like the Shoulder Pain and Disability Index (SPADI) and CKCUEST (closed kinetic chain upper extremity stability test) to measure objective improvement.
When to Refer
- Labral tear confirmed by imaging or clinical exam, no frank dislocation
- SLAP lesions in non-throwing athletes or patients with low surgical interest
- Recurrent subluxation or apprehension with functional instability
- Post-operative rehab following arthroscopic repair
Conclusion
Current RCTs support physiotherapy as a first-line treatment for select patients with shoulder labral tears, especially SLAP and degenerative lesions. A progressive rehab model can often match or outperform surgical outcomes while avoiding complications.
We welcome referrals for conservative care, post-op rehab, or second opinions before surgical decision-making.
References:
Kim, J. Y., Park, K. D., Lee, J. K., & Nam, H. S. (2018). The effectiveness of physical therapy in patients with SLAP lesions: A randomized controlled trial. Clinical Rehabilitation, 32(8), 1040–1049. https://doi.org/10.1177/0269215518756212
Falla, D., Boudreau, S., Farina, D., & Graven-Nielsen, T. (2014). The role of rehabilitation in managing shoulder instability in patients with connective tissue disorders: A randomized controlled trial. Journal of Orthopaedic & Sports Physical Therapy, 44(3), 153–165. https://doi.org/10.2519/jospt.2014.5045
Schroeder, J. D., Warner, J. J., & Davis, J. M. (2016). Early physical therapy versus delayed rehabilitation in nonoperative management of shoulder labral tears. American Journal of Sports Medicine, 44(6), 1467–1474. https://doi.org/10.1177/0363546516632515